
Northwest women say that almost half of their pregnancies are mistimed or unwanted.
In contrast with Europe and Canada, the Pacific Northwest faces an epidemic of surprise pregnancy. Northwest women say that almost half of their pregnancies are mistimed or unwanted. This causes hardship in the lives of the region’s families and makes it difficult to give children the best possible start in life. With unintended pregnancy so common and the consequences so big, the American College of Obstetricians and Gynecologists now recommends that health care providers check pregnancy desires at every visit with reproductive-age women and, when appropriate, offer “whoops-proof” IUDs and implants that work 20 times better than the pill.
But pressures on providers make this tough. Clinicians are swamped with ever more tasks and topics to cover and ever smaller chunks of time in which to address them all. Even those who would prefer a whole-person approach often don’t know whether and when a patient might want to have a kid, which means they can’t help a prospective parent prepare for healthy babies. Now, a small Oregon non-profit has come up with a simple innovation may change that.
One Key Question
The Oregon Foundation for Reproductive Health, based in Portland, developed a remarkably simple screening technique called One Key Question® (OKQ). It fits into busy schedules and can be completed by clinic assistants—or maybe eventually a waiting room app. The one key question is this: “Would you like to become pregnant in the next year?” The clinician documents one of four patient responses: Yes, I’m okay either way, I’m not sure, or No, which then guides next steps.
Patients who say yes receive preconception counseling about how they can stack the odds in favor of a healthy pregnancy by improving nutrition, avoiding toxins, and addressing chronic conditions or stress. Patients who feel uncertain or ambivalent (I don’t know or I’m okay either way) get information about preconception care as well as family planning options. A response of no leads to just the conversation about family planning. It creates an opportunity to check satisfaction with a patient’s current method and explore methods like IUDs and implants that might better fit patient goals but are less familiar. Inexpensive posters and tear sheets from the National Campaign to Prevent Teen and Unintended Pregnancy and a color-coded medical eligibility chart from the CDC make it easy for providers to walk a patient through the options.
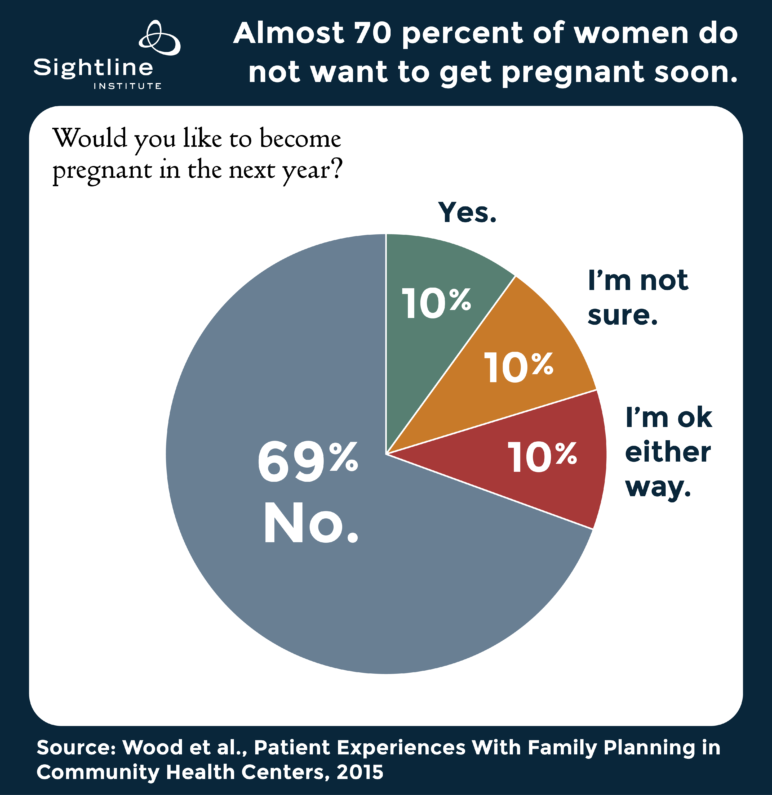
As shown in the figure below, of 1,847 US women asked One Key Question in a 2015 study, almost seven in ten women responded to One Key Question with “no.” Ten percent each responded with “yes,” “I’m not sure,” or “I’m okay either way.”
Promising beginnings
Although One Key Question is relatively new, early feedback from clinicians looks promising, and it has caught the attention of experts nationwide. One example is the state of Delaware, where Governor Jack Markell partnered with Upstream USA to retool contraceptive care statewide, so that women can receive the method of their choice on the same day, free of charge—including IUDs and implants. The statewide contraceptive care upgrade, called Delaware CAN, has trained caregivers serving over 50,000 women in 60 different clinical settings.
In Oregon, OKQ is deployed in a variety of settings, from home visits and food assistance to primary care. A pilot project at One Community Health compared two major health centers, one in which OKQ was implemented and one in which it was not. After just one month, 64 percent of electronic medical records for the OKQ-practicing site documented appropriate screening for pregnancy desires, compared to 12 percent at the non-OKQ site.
Challenges remain
Even clinicians who would like to improve reproductive outcomes for their patients will need evidence that adopting a screening protocol such as One Key Question will make patient care easier in the long run, and more satisfying—rather than simply adding one more thing to an already overwhelming to-do list.
Cultural dynamics create a different type of challenge. Sexuality and reproduction can be sensitive topics for providers as well as patients. In particular, those women who are young, poor, ethnic minorities, or in ill health can feel shamed or pressured unless conversations are carefully client-centered. That said, a strong majority do not want to get pregnant in the next year, and many women say that they appreciate being asked.
Health centers that want to use OKQ in a systematic and routine way face logistical challenges incorporating the OKQ algorithm into varying electronic health records. In Oregon, OCHIN, a company providing health information technology, has incorporated the question and answers into the EPIC electronic record used across their network. But other systems use other platforms, so not all providers would get prompted to make a simple note of a woman’s pregnancy intentions.
Keys to success
To ensure program excellence and compatibility of evaluation across settings, the non-profit Oregon Foundation for Reproductive Health trademarked One Key Question and asks for a signed memorandum of understanding prior to implementation. In settings that have adopted OKQ, success tends to follow a specific set of best practices. These include training the whole health center team prior to roll-out, adjusting workflow, updating protocols and referral lists for preconception or family-planning care, and building a plan to evaluate impact.
Of course, it only makes sense to ask about what people want if clinicians then have services to offer. One Key Question can reveal gaps in service capacity that require other kinds of staff training or upgrades in the healthcare system as a whole. Fortunately, several great models show how it can be done. I recently wrote about the Colorado Initiative to Reduce Unintended Pregnancy, which dramatically reduced teen pregnancy and abortion by improving access to implants and IUDs. Delaware, which once had the highest rate of unintended pregnancy in the country, is now making similar changes with help from Upstream USA. The “Beyond the Pill” program at University of California San Francisco offers onsite trainings to individual clinics wanting to upgrade contraceptive services, with grant funding for those that qualify.
No change is effortless, but some changes make life easier and better in the long run, and this seems to be one of them.
To learn more about One Key Question or to sign up for a monthly newsletter, please contact info@onekeyquestion.org.

{kind=link}
4 thoughts on “Would you like to have a kid in the next year?”
Comments are closed.